
FAQs
Welcome to the M.A.G.I.C. Clinic
Genetics is a constantly changing and rapidly advancing field. Many patients can wait years to get a diagnosis. The number of ways to obtain a genetic diagnosis is complex. The approach used at M.A.G.I.C. Clinic is unique – our goal is to try to find a diagnosis using the fastest possible approach so that any treatment, if available, can be started as early as possible. There is a complicated menu of tests: some are offered by the public system and others are private tests. Whole Genome Sequencing (WGS) is a major advance that has simplified the approach to look for a rare metabolic or genetic disease and can reduce the time it takes to make a diagnosis for the majority of genetic diseases. Our laboratory, Discovery DNA, was the first laboratory in Alberta to offer diagnostic-grade WGS back in 2021. We use the best science from the peer-reviewed literature to inform our approach and make our recommendations.
Referral FAQs
We ask that you be informed as possible about your reason for referral to our clinic, be aware of the approach we use, and have some information about expectations when you come to our clinic. We have found that patients find it useful to list their personal goals for the consultation so that we can better understand your needs. Our goal is to do our best to look after you or your loved one and to make the consultation serve the purpose of improving health care outcomes.
1. Do I need a referral / consultation to be seen at M.A.G.I.C. Clinic?
- Yes, a referral from another healthcare provider is required. There are exceptions for certain situations during pregnancy (such as NIPS or a fetal anomaly on ultrasound), or outside of a pregnancy where an urgent metabolic or genetic diagnosis is needed (such as Hurler syndrome or metachromatic leukodystrophy – there are many others). The referral must clearly state what the consultation request is for. Other conditions may apply. We are not a primary care clinic.
- We accept referrals for cases within our scope of practice and where we think our service can be helpful. We do not accept referrals for the following:
- Hypermobility. Please use Hypermobility Canada for these referrals (both Pediatric and Adult).
- Self-Diagnosed conditions using the internet or AI. We know it’s out there – our experience is that in the specialty we practice, it is not the way to start. It’s best to see your primary health care provider first to see if it makes sense.
- General interest in consultation with no differential from the person requesting the consult.
- Folate antibody testing for autism. We will not order testing or provide prescriptions for folinic acid for this indication.
- To order testing (whether public or private) on behalf of another practitioner or consumer-directed.
- Patients who are awaiting referral to, have test results pending at, or are currently being followed by another geneticist. We do accept transfer of care and formal second opinions.
- To interpret or take action on genetic test results that were not part of a clinically-directed workup, such as many direct-to-consumer tests, or from labs that have not traditionally been involved in providing a genetic diagnosis.
- To get general information about something. We are a medical clinic meaning there has to be a medical need and a patient in need of a medical service.
2. What is the wait time?
- Wait times vary by the type of referral. There are urgent referrals – such as a pregnant patient or a patient where their medical condition requires urgency which will be triaged and seen on a priority basis. It is important that patients complete the pre-booking requirements. Pre-booking requirements need to be completed to avoid the referral then being closed. It is important that you pay attention to your email and complete the requirements when you receive notification to do these.
3. Is there a charge for the referral / consultation?
- Consultation requests with a medical doctor that meet the referral requirements are not charged for the consultation. The patient is required to have coverage by public health insurance by their province in Canada with the exception of patients who have health care coverage through the province of Quebec. This difference is because of reciprocal agreements between provinces which can vary from province to province. For in-person referrals for patients with provincial insurance through the province of Quebec or who don’t have provincial health care coverage, patients will be billed directly for medical services. The billing fee code in Alberta is generally used to determine the amount but can vary. You can ask about the estimated billing amount prior to your appointment. You may, on your own, seek reimbursement of the costs from your insurance provider.
4. Will I get billed for Telehealth services?
- Telehealth services are not covered the same way as in-person services. Telehealth services are also governed by medical licensing restrictions in different provinces and our medical staff have to abide by those regulations. Unless there is the ability to provide Telehealth insurances through the patient’s health plan, Telehealth services are billed directly to the patient. It may be that the cost of Telehealth is lower than the cost of your travel for an in-person visit and depending on the reason for the consultation, Telehealth may be an option for some patients. For referrals to our clinic in Calgary, Telehealth for patients within Alberta who have Alberta health care coverage are generally the ones not billed to patients. Because of licensing restrictions, initial consultations for Telehealth outside for patients outside Alberta, Saskatchewan, British Columbia or the Yukon cannot be accepted. You may be able to apply to your health care provider for reimbursement of charges on your own. It sounds complicated and it is complicated because of regulations and rules we have to follow. You will be informed whether billing applies prior to setting up an appointment.
5. What type of patients are seen at M.A.G.I.C. Clinic?
- M.A.G.I.C. Clinic specializes in diseases (affecting both children and adults) that either have or may have a metabolic basis (such as inborn errors of metabolism) or genetic basis (such as genetic diseases). The focus on undiagnosed cases is to try to find a diagnosis. This strategy will vary based on the type of patient and the best available medical evidence. The strategy for investigations is determined by the consultation. The strategy may involve using available publicly funded tests (such as blood and urine tests, certain genetic tests, ordering imaging and X-rays, performing procedures such as lumbar puncture or muscle biopsy) or private testing (such as whole genome sequencing and other tests). The goal is to identify whether there is a medical diagnosis. We are not a consumer-demand clinic. This means the tests ordered are determined by the clinician in consultation with the patient/care provider but not are not ordered simply because there is a request to order them from the patient or other person. We also do not use an approach to simply order the public tests first to see if something can be found – it’s possible public tests (or private tests) can have significant limitations and tests with significant limitations are unlikely to be the ones that meet a recommendation. Patients are not required to undergo any testing they don’t want to have done. The purpose of the consultation is to advise which tests, in any, can provide a diagnosis. You can take the advice and decide exactly how you want to proceed with M.A.G.I.C. Clinic or get an opinion from another clinic if you wish. We do not order tests simply because they are available.
- The second major group of services are treatments for rare metabolic or genetic diseases. There are a limited number of diseases for which treatments are covered by provincial health insurance. If it is within our scope, we may initiate treatment or advise you of any options that may exist.
6. What types of genetic testing are available?
- We have about 20,000 pairs of genes (one set from each parent). The genes are very small and are made up of DNA. Strings of DNA are wrapped into larger structures called chromosomes. Humans have 23 pairs of chromosomes – they are numbered from 1-22 and the 23 pair are the sex chromosomes (the composition usually being XX in females or XY in males by sex at birth).
- The genetic testing strategy depends on the question that needs to be answered and patient characteristics. Some tests, such as chromosomal analysis, certain genetic panels, screening for inborn errors of metabolism, testing for hereditary cancer, may be available through public testing and we consider these options if they are suitable. Out-of-province patients are not always eligible for certain tests when the testing is ordered in a different province; and in general, genetic testing is not covered for out-of-province patients.
- When looking for a rare metabolic or genetic disease, testing comes down to the following general choices:
- Chromosomal Microarray (CMA) – looks for major changes in large regions of chromosomes. This is a general first line test when there is major intellectual or developmental delay or congenital anomalies. We prefer the CMA be ordered by your doctor before the referral is made. If there abnormalities on the CMA then we get involved to help sort these out as part of consultation. Testing must meet provincial criteria but this is a publicly covered test.
- Copy number variant (CNV) or imprinting condition. Examples include Fragile X, Prader-Willi syndrome and others. These are specialized tests that are ordered when the clinical picture indicates a high index of suspicion for specific disorders.
- Gene Panel. A gene panel is a limited list of genes (for example 50 genes out of the 20,000) which is ordered when a gene for a particular disease is in the list of these genes. Gene panels vary from lab to lab. Not all types of disease presentations have a gene panel. There are gene panels which are in house (run by Alberta labs) or gene panels that sometimes have to be sent out-of-province. Because of the limited number of genes, gene panels are not the most comprehensive test for an undiagnosed rare disease. A gene that may be the diagnosis in a patient may not be on the gene panel. For certain issues, like congenital hearing loss, some gene panels might be a good place to start. For things like intellectual delay or autism, a gene panel will have a lower yield than whole genome sequencing. For this reason, unless we have a very strong index of suspicion that we will find a gene for a particular feature, we do not order gene panels. Gene panels must meet provincial criteria but are generally covered by public testing. Keep in mind, we do not order a gene panel simply because it is a publicly covered test if, in our opinion, this is not the best approach to finding a diagnosis.
- Genomic Testing. This boils down to 2 types of tests – Whole Exome Sequencing (WES) or Whole Genome Sequencing (WGS).
- Genes are arranged as exons (coding regions) and introns (non-coding regions). Changes in either the exons or introns can result in a genetic disease.
- WES (Whole Exome Sequencing). Exomes are the coding regions of genes. About 80-85% of genetic diseases are diagnosed by sequencing the exons but this only covers about 1.5% of DNA (the result are introns). Our laboratory, Discovery DNA, was the first laboratory in Alberta to offer clinical-grade WES but that was more than 5 years ago and we have replaced this with WGS. We no longer order WES as a general screen for genetic diseases. While there is a provincial program to do WES, we recommend that you see a geneticist who will order WES if you want to use this approach.
- WGS (Whole Genome Sequencing). A genome includes all of the exons plus the introns. It is as close to sequencing 100% of the DNA as we can get. WGS is surpassing WES as the standard first tier test for undiagnosed metabolic or genetic diseases in many different parts of the world including at M.A.G.I.C. Clinic. The chance of finding a diagnosis is higher with WGS compared to WES. While WGS is a private test, this is the preferred method to screen for an undiagnosed disease at M.A.G.I.C. Clinic.
- Our approach is to use the most comprehensive tool as the first tool – which is WGS. We do not use an approach to simply run through all the publicly available tests first before going to WGS. We suggest using another clinic for that approach.
- For some types of testing, there can be considerable time and effort required to complete applications to determine whether a patient qualifies for a public test. This extra work is not remunerated to the clinic and can be significant. For genetic testing using whole exome or whole genome sequencing (WES/WGS), it’s important that we have access to the raw data and use labs with experience in interpreting this data for diagnostic purposes. Because of these reasons and the nature of interpreting and reporting genomic test results, our approach for genomic testing is to use a private test that we are familiar with, either through our affiliated provider, Discovery DNA, or similar lab that meets the conditions above. Patients may find different choices through another clinic and are free to engage in those services if they choose not to have WGS through our clinic. Our preferred large scale test is WGS and WES is only ordered if there is a specific reason why it might be more suitable. It is important that patients / care providers understand that when the goal is to determine whether a rare metabolic or generic disease exists or does not exist, it is the interpretation of the data and not simply a report that matters. Our approach is to use the methods with the highest confidence in providing an answer. We place a high priority in providing an interpretation of the results and helping direct the next decisions rather than simply running a series of tests.
- You may find the following article has more information
7. What is the role of whole genome sequencing (WGS) in making a diagnosis?
- It is important to understand that our approach is directed to reduce the time to make a diagnosis and our primary genomic test is WGS which is a private test. There is no public coverage for WGS but some health insurance plans may provide coverage.
- A common consultation request may be to ask us find a diagnosis for a rare metabolic or genetic disease due to certain issues, like epilepsy, poor growth, autism, areas of the body that aren’t function properly (such as congenital heart lesion, hypertrophic cardiomyopathy, long QT syndromes) , the brain (such as structural abnormalities). There are more than 7,000 rare diseases and if there is no obvious answer, then WGS is currently the test advised by many medical societies as the first tier test to try and make a diagnosis. While WGS is a private test, it has many advantages compared to traditional approaches that only test a few genes at a time, or require blood, urine, spinal fluid collection, imaging or even tissue biopsy. WGS looks at the coding (exons) and non-coding regions (introns) of pretty much all of the 20,000 pairs of genes that humans have. A WGS test does 50 has more sequencing than an exome so it costs more. But WGS can be done on a non-invasive sample (like a cheek swab or saliva), generates data to look for other areas of interest, provides a better chance at determining copy number variants of certain genes and looking at those non-coding regions which can sometimes cause a rare genetic disease. We analyze the data on WGS using international standards and the experience we have developed in trying to find answers. This is why it’s important for us to have the data. We provide the interpretation of the data to let you know whether or not a diagnosis can be made.
- Metabolic and Genetic diseases are rare and all together can affect about 10% of the population. This means most people who have a WGS test done will not have a known rare disease. It is important to understand that a negative WGS result may mean there is nothing, in terms of a genetic diagnosis even though health may still be affected. Not all diseases have a genetic basis and our current knowledge and technology has limitations.
- WGS is a private test. In some cases, a different type of test may be needed so it’s not necessary that all patients get an WGS. The reasons for doing a WGS are based on the consultation. While you can order a WGS on your own or through your doctor through Discovery DNA, M.A.G.I.C. Clinic only makes a WGS recommendation with a consultation. It may be that a WGS is not required to make a diagnosis and that another test, which may be covered publicly, is the recommendation provided. Currently, WGS is recommended in less than 10% of all referred cases. The recommendation is specific to the patient and only determined after the consultation.
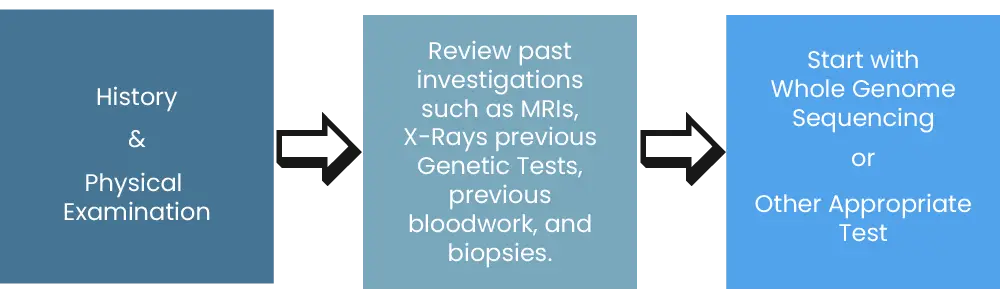
- Our goal is to reduce the time it takes to make a diagnosis and the most common approach, based on the best available evidence, one may expect is in the following diagram:
8. Does M.A.G.I.C. Clinic see patients with Hypermobility?
- New referrals for Hypermobility and related issues are now seen through a dedicated clinic called Hypermobility Canada. M.A.G.I.C. Clinic is no longer accepting referrals for hypermobility / Ehler-Danlos syndromes, POTS (postural orthostatic tachycardia, or MCAS (mast cell activation syndrome).
- Please do not refer patients with hypermobility or suspected Ehler-Danlos syndrome to M.A.G.I.C. Clinic – these will all be declined.
9. Can I get follow-up care?
- In general, a consultation request is to get an opinion and not for ongoing care. However, if a diagnosis is made and the type of care is within our scope of practice, we will discuss treatment options and offer follow-up.
10. What about referrals for a personal or family history of cancer?
- Hereditary Cancer is an important part of what we do and we do accept referrals for genetic testing when a patient either has a certain type of cancer or has a concerning family history of cancer.
- The core service is genetic consultation. We value the role of genetic counselling and this may sometimes be the main reason for the consultation.
- There is genetic testing that varies province by province. For patients in Alberta that come to our Calgary clinic, there are requirements to qualify for a public test. We use this option when we think it’s very likely that public testing will be covered. All other situations will most likely require a private test. Depending on the information provided at the time of referral, we may book and appointment in Calgary as long as you understand it may be a private test that is available or redirect the referral to a particular pathway in your home province.
- If you have a family member who has had genetic testing, you must send us a copy of the lab report, and complete a family history using a tool we provide, in order to get an appointment.
11. My child had a report on a chromosomal microarray indication absence of heterozygosity (AOH). What services does your clinic provide?
- The finding of AOH (absence of heterozygosity) means there are genes that look identical (for most people, the genetic codes are not identical because each set was inherited from a mother and father who are not related to each other).
- Within the regions of AOH, there could be regions of identical genes that cause an abnormality in an individual – autism seems to be the most frequent referral we get with this indication.
- Finding whether there are any identical genes that cause a diagnosis is not an easy task and requires techniques not covered by public testing. Our approach is to do whole genome sequencing (WGS) in an individual with this AOH finding and then sort through the regions (there can be millions in some cases) to see if we can find a set of genes that explain what is going on.
- We require that all referring providers and the parents/care providers understand that there will be a private cost to come to an answer in all circumstances. Appointments are only booked where we have documentation that this is understood. We don’t want parents / care providers waiting a long time for an appointment to only find out about this later.
12. What is your workup for autism?
- Our focus is to look for genetic causes of autism (or related disorders like autism spectrum disorder) that has already been diagnosed.
- An increasing number of genetic syndromes are ultimately being found to be a cause of autism
- The typical practice is to start with a chromosomal microarray first (CMA). Sometimes fragile X testing is ordered if criteria are met. We ask that any of these tests, as decided by the referring doctor, be completed prior to referring to M.A.G.I.C.. If the results are positive or can’t be explained by the ordering physician then we will take the referral to explain abnormal results. In many cases, abnormal results from a CMA do not explain why a person has autism. A larger number of cases can be diagnosed using WGS. This means for the majority of people with autism, the approach through our clinic will be WGS. The purpose of running any test is to provide you with the best interpretation we can and not simply to run ‘a test’. We analyze the data from WGS before reporting it out. It’s important to understand that this is a different approach than most clinics and is aimed at being as comprehensive as possible. Without the right information, it’s not possible to draw the right conclusion. We do not order whole exome sequencing (WES) or gene panels as a general screen for genetic causes of autism. We also do not order testing, public or private, where we are not provided the raw sequencing data or from a lab that has not been traditionally involved in using this type of technology to make a genetic diagnosis.
- If you are a couple with a child with autism for which there is no genetic diagnosis and you are wondering whether there is a higher risk of having another child with autism, in general there is a higher risk but the percentage risk can vary depending on whether or not there is a genetic diagnosis. Prenatal testing is only possible in another pregnancy if a genetic cause has been identified. We require that the referring HCP discuss this with their patients and only accept referrals where there an interest in pursuing a genetic diagnosis.
- We are not a clinic that will diagnose autism. A specialist in autism, such as a neurodevelopmental pediatrician or psychologist, should be seen for that purpose. Our focus is trying to identify whether there is a genetic cause of autism with or without other neurodevelopmental issues.
- We do not order testing for folate receptor antibodies or prescribe folinic acid for these purposes. Our opinion is that the science behind this is not well developed enough yet to take this approach.
- If a referral is declined, it is generally because it was not understood whether the goal of the referral fits in with this scope or whether this was communicated to the patient or care providers.
13. What evaluation do you offer during pregnancy?
- Consultations during pregnancy are handled as a priority. We will accept self-referrals for pregnancy depending on the circumstances.
- The following are our primary services in pregnancy:
- Non-Invasive prenatal screening (NIPS) which is a private test. The cost is for the test only. The consultation is covered by the insurance provider with the conditions as described above under the FAQ for consultations.
- Medical Genetics consultation for fetal anomalies or genetic diseases affecting the pregnancy – whether the mother has or is considered to have a genetic disease or the baby. Examples of a mother’s genetic disease can include homocystinuria. Examples of fetal anomalies can include absence of a limb on fetal ultrasound. There is no fee for the consultation (same conditions as a general consultation) but there are certain tests that may not be publicly covered (such as WGS on an amniocentesis sample) which would be at a private cost if chosen. Other types of tests, like fetal karyotyping, are covered by public services and we will arrange and order them as indicated.
- Arranging for invasive prenatal testing using chorionic villus sampling or amniocentesis if the pregnancy is at risk for a metabolic or genetic disease.
- Pre-pregnancy screening for genetic diseases in the couple considering a pregnancy. The approach will be customized to the situation. For example, screening for thalassemia may be done through public testing if it meets the public testing conditions. We do offer WGS carrier screening for couples as a private test.
14. What about services like nursing, genetic counselling or pharmacy consultation?
- Registered nurses, genetic counsellors and pharmacists are professionals in their own right however there is no public coverage for these services – the services will be billed directly to the patient
- If one of these professionals is involved in the initial consultation, they will help set up requisitions for bloodwork or imaging as part of the initial consultation without a charge but any additional services, such as answering emails, telephone requests, medical advice will be billed directly to the patient
1. Do I need a referral / consultation to be seen at M.A.G.I.C. Clinic?
- Yes, a referral from another healthcare provider is required. There are exceptions for certain situations during pregnancy (such as NIPS or a fetal anomaly on ultrasound), or outside of a pregnancy where an urgent metabolic or genetic diagnosis is needed (such as Hurler syndrome or metachromatic leukodystrophy – there are many others). The referral must clearly state what the consultation request is for. Other conditions may apply. We are not a primary care clinic.
- We accept referrals for cases within our scope of practice and where we think our service can be helpful. We do not accept referrals for the following:
- Hypermobility. Please use Hypermobility Canada for these referrals (both Pediatric and Adult).
- Self-Diagnosed conditions using the internet or AI. We know it’s out there – our experience is that in the specialty we practice, it is not the way to start. It’s best to see your primary health care provider first to see if it makes sense.
- General interest in consultation with no differential from the person requesting the consult.
- Folate antibody testing for autism. We will not order testing or provide prescriptions for folinic acid for this indication.
- To order testing (whether public or private) on behalf of another practitioner or consumer-directed.
- Patients who are awaiting referral to, have test results pending at, or are currently being followed by another geneticist. We do accept transfer of care and formal second opinions.
- To interpret or take action on genetic test results that were not part of a clinically-directed workup, such as many direct-to-consumer tests, or from labs that have not traditionally been involved in providing a genetic diagnosis.
- To get general information about something. We are a medical clinic meaning there has to be a medical need and a patient in need of a medical service.
2. What is the wait time?
- Wait times vary by the type of referral. There are urgent referrals – such as a pregnant patient or a patient where their medical condition requires urgency which will be triaged and seen on a priority basis. It is important that patients complete the pre-booking requirements. Pre-booking requirements need to be completed to avoid the referral then being closed. It is important that you pay attention to your email and complete the requirements when you receive notification to do these.
3. Is there a charge for the referral / consultation?
- Consultation requests with a medical doctor that meet the referral requirements are not charged for the consultation. The patient is required to have coverage by public health insurance by their province in Canada with the exception of patients who have health care coverage through the province of Quebec. This difference is because of reciprocal agreements between provinces which can vary from province to province. For in-person referrals for patients with provincial insurance through the province of Quebec or who don’t have provincial health care coverage, patients will be billed directly for medical services. The billing fee code in Alberta is generally used to determine the amount but can vary. You can ask about the estimated billing amount prior to your appointment. You may, on your own, seek reimbursement of the costs from your insurance provider.
4. Will I get billed for Telehealth services?
- Telehealth services are not covered the same way as in-person services. Telehealth services are also governed by medical licensing restrictions in different provinces and our medical staff have to abide by those regulations. Unless there is the ability to provide Telehealth insurances through the patient’s health plan, Telehealth services are billed directly to the patient. It may be that the cost of Telehealth is lower than the cost of your travel for an in-person visit and depending on the reason for the consultation, Telehealth may be an option for some patients. For referrals to our clinic in Calgary, Telehealth for patients within Alberta who have Alberta health care coverage are generally the ones not billed to patients. Because of licensing restrictions, initial consultations for Telehealth outside for patients outside Alberta, Saskatchewan, British Columbia or the Yukon cannot be accepted. You may be able to apply to your health care provider for reimbursement of charges on your own. It sounds complicated and it is complicated because of regulations and rules we have to follow. You will be informed whether billing applies prior to setting up an appointment.
5. What type of patients are seen at M.A.G.I.C. Clinic?
- M.A.G.I.C. Clinic specializes in diseases (affecting both children and adults) that either have or may have a metabolic basis (such as inborn errors of metabolism) or genetic basis (such as genetic diseases). The focus on undiagnosed cases is to try to find a diagnosis. This strategy will vary based on the type of patient and the best available medical evidence. The strategy for investigations is determined by the consultation. The strategy may involve using available publicly funded tests (such as blood and urine tests, certain genetic tests, ordering imaging and X-rays, performing procedures such as lumbar puncture or muscle biopsy) or private testing (such as whole genome sequencing and other tests). The goal is to identify whether there is a medical diagnosis. We are not a consumer-demand clinic. This means the tests ordered are determined by the clinician in consultation with the patient/care provider but not are not ordered simply because there is a request to order them from the patient or other person. We also do not use an approach to simply order the public tests first to see if something can be found – it’s possible public tests (or private tests) can have significant limitations and tests with significant limitations are unlikely to be the ones that meet a recommendation. Patients are not required to undergo any testing they don’t want to have done. The purpose of the consultation is to advise which tests, in any, can provide a diagnosis. You can take the advice and decide exactly how you want to proceed with M.A.G.I.C. Clinic or get an opinion from another clinic if you wish. We do not order tests simply because they are available.
- The second major group of services are treatments for rare metabolic or genetic diseases. There are a limited number of diseases for which treatments are covered by provincial health insurance. If it is within our scope, we may initiate treatment or advise you of any options that may exist.
6. What types of genetic testing are available?
- We have about 20,000 pairs of genes (one set from each parent). The genes are very small and are made up of DNA. Strings of DNA are wrapped into larger structures called chromosomes. Humans have 23 pairs of chromosomes – they are numbered from 1-22 and the 23 pair are the sex chromosomes (the composition usually being XX in females or XY in males by sex at birth).
- The genetic testing strategy depends on the question that needs to be answered and patient characteristics. Some tests, such as chromosomal analysis, certain genetic panels, screening for inborn errors of metabolism, testing for hereditary cancer, may be available through public testing and we consider these options if they are suitable. Out-of-province patients are not always eligible for certain tests when the testing is ordered in a different province; and in general, genetic testing is not covered for out-of-province patients.
- When looking for a rare metabolic or genetic disease, testing comes down to the following general choices:
- Chromosomal Microarray (CMA) – looks for major changes in large regions of chromosomes. This is a general first line test when there is major intellectual or developmental delay or congenital anomalies. We prefer the CMA be ordered by your doctor before the referral is made. If there abnormalities on the CMA then we get involved to help sort these out as part of consultation. Testing must meet provincial criteria but this is a publicly covered test.
- Copy number variant (CNV) or imprinting condition. Examples include Fragile X, Prader-Willi syndrome and others. These are specialized tests that are ordered when the clinical picture indicates a high index of suspicion for specific disorders.
- Gene Panel. A gene panel is a limited list of genes (for example 50 genes out of the 20,000) which is ordered when a gene for a particular disease is in the list of these genes. Gene panels vary from lab to lab. Not all types of disease presentations have a gene panel. There are gene panels which are in house (run by Alberta labs) or gene panels that sometimes have to be sent out-of-province. Because of the limited number of genes, gene panels are not the most comprehensive test for an undiagnosed rare disease. A gene that may be the diagnosis in a patient may not be on the gene panel. For certain issues, like congenital hearing loss, some gene panels might be a good place to start. For things like intellectual delay or autism, a gene panel will have a lower yield than whole genome sequencing. For this reason, unless we have a very strong index of suspicion that we will find a gene for a particular feature, we do not order gene panels. Gene panels must meet provincial criteria but are generally covered by public testing. Keep in mind, we do not order a gene panel simply because it is a publicly covered test if, in our opinion, this is not the best approach to finding a diagnosis.
- Genomic Testing. This boils down to 2 types of tests – Whole Exome Sequencing (WES) or Whole Genome Sequencing (WGS).
- Genes are arranged as exons (coding regions) and introns (non-coding regions). Changes in either the exons or introns can result in a genetic disease.
- WES (Whole Exome Sequencing). Exomes are the coding regions of genes. About 80-85% of genetic diseases are diagnosed by sequencing the exons but this only covers about 1.5% of DNA (the result are introns). Our laboratory, Discovery DNA, was the first laboratory in Alberta to offer clinical-grade WES but that was more than 5 years ago and we have replaced this with WGS. We no longer order WES as a general screen for genetic diseases. While there is a provincial program to do WES, we recommend that you see a geneticist who will order WES if you want to use this approach.
- WGS (Whole Genome Sequencing). A genome includes all of the exons plus the introns. It is as close to sequencing 100% of the DNA as we can get. WGS is surpassing WES as the standard first tier test for undiagnosed metabolic or genetic diseases in many different parts of the world including at M.A.G.I.C. Clinic. The chance of finding a diagnosis is higher with WGS compared to WES. While WGS is a private test, this is the preferred method to screen for an undiagnosed disease at M.A.G.I.C. Clinic.
- Our approach is to use the most comprehensive tool as the first tool – which is WGS. We do not use an approach to simply run through all the publicly available tests first before going to WGS. We suggest using another clinic for that approach.
- For some types of testing, there can be considerable time and effort required to complete applications to determine whether a patient qualifies for a public test. This extra work is not remunerated to the clinic and can be significant. For genetic testing using whole exome or whole genome sequencing (WES/WGS), it’s important that we have access to the raw data and use labs with experience in interpreting this data for diagnostic purposes. Because of these reasons and the nature of interpreting and reporting genomic test results, our approach for genomic testing is to use a private test that we are familiar with, either through our affiliated provider, Discovery DNA, or similar lab that meets the conditions above. Patients may find different choices through another clinic and are free to engage in those services if they choose not to have WGS through our clinic. Our preferred large scale test is WGS and WES is only ordered if there is a specific reason why it might be more suitable. It is important that patients / care providers understand that when the goal is to determine whether a rare metabolic or generic disease exists or does not exist, it is the interpretation of the data and not simply a report that matters. Our approach is to use the methods with the highest confidence in providing an answer. We place a high priority in providing an interpretation of the results and helping direct the next decisions rather than simply running a series of tests.
- You may find the following article has more information
7. What is the role of whole genome sequencing (WGS) in making a diagnosis?
- It is important to understand that our approach is directed to reduce the time to make a diagnosis and our primary genomic test is WGS which is a private test. There is no public coverage for WGS but some health insurance plans may provide coverage.
- A common consultation request may be to ask us find a diagnosis for a rare metabolic or genetic disease due to certain issues, like epilepsy, poor growth, autism, areas of the body that aren’t function properly (such as congenital heart lesion, hypertrophic cardiomyopathy, long QT syndromes) , the brain (such as structural abnormalities). There are more than 7,000 rare diseases and if there is no obvious answer, then WGS is currently the test advised by many medical societies as the first tier test to try and make a diagnosis. While WGS is a private test, it has many advantages compared to traditional approaches that only test a few genes at a time, or require blood, urine, spinal fluid collection, imaging or even tissue biopsy. WGS looks at the coding (exons) and non-coding regions (introns) of pretty much all of the 20,000 pairs of genes that humans have. A WGS test does 50 has more sequencing than an exome so it costs more. But WGS can be done on a non-invasive sample (like a cheek swab or saliva), generates data to look for other areas of interest, provides a better chance at determining copy number variants of certain genes and looking at those non-coding regions which can sometimes cause a rare genetic disease. We analyze the data on WGS using international standards and the experience we have developed in trying to find answers. This is why it’s important for us to have the data. We provide the interpretation of the data to let you know whether or not a diagnosis can be made.
- Metabolic and Genetic diseases are rare and all together can affect about 10% of the population. This means most people who have a WGS test done will not have a known rare disease. It is important to understand that a negative WGS result may mean there is nothing, in terms of a genetic diagnosis even though health may still be affected. Not all diseases have a genetic basis and our current knowledge and technology has limitations.
- WGS is a private test. In some cases, a different type of test may be needed so it’s not necessary that all patients get an WGS. The reasons for doing a WGS are based on the consultation. While you can order a WGS on your own or through your doctor through Discovery DNA, M.A.G.I.C. Clinic only makes a WGS recommendation with a consultation. It may be that a WGS is not required to make a diagnosis and that another test, which may be covered publicly, is the recommendation provided. Currently, WGS is recommended in less than 10% of all referred cases. The recommendation is specific to the patient and only determined after the consultation.
- Our goal is to reduce the time it takes to make a diagnosis and the most common approach, based on the best available evidence, one may expect is in the following diagram:
8. Does M.A.G.I.C. Clinic see patients with Hypermobility?
- New referrals for Hypermobility and related issues are now seen through a dedicated clinic called Hypermobility Canada. M.A.G.I.C. Clinic is no longer accepting referrals for hypermobility / Ehler-Danlos syndromes, POTS (postural orthostatic tachycardia, or MCAS (mast cell activation syndrome).
- Please do not refer patients with hypermobility or suspected Ehler-Danlos syndrome to M.A.G.I.C. Clinic – these will all be declined.
9. Can I get follow-up care?
- In general, a consultation request is to get an opinion and not for ongoing care. However, if a diagnosis is made and the type of care is within our scope of practice, we will discuss treatment options and offer follow-up.
10. What about referrals for a personal or family history of cancer?
- Hereditary Cancer is an important part of what we do and we do accept referrals for genetic testing when a patient either has a certain type of cancer or has a concerning family history of cancer.
- The core service is genetic consultation. We value the role of genetic counselling and this may sometimes be the main reason for the consultation.
- There is genetic testing that varies province by province. For patients in Alberta that come to our Calgary clinic, there are requirements to qualify for a public test. We use this option when we think it’s very likely that public testing will be covered. All other situations will most likely require a private test. Depending on the information provided at the time of referral, we may book and appointment in Calgary as long as you understand it may be a private test that is available or redirect the referral to a particular pathway in your home province.
- If you have a family member who has had genetic testing, you must send us a copy of the lab report, and complete a family history using a tool we provide, in order to get an appointment.
11. My child had a report on a chromosomal microarray indication absence of heterozygosity (AOH). What services does your clinic provide?
- The finding of AOH (absence of heterozygosity) means there are genes that look identical (for most people, the genetic codes are not identical because each set was inherited from a mother and father who are not related to each other).
- Within the regions of AOH, there could be regions of identical genes that cause an abnormality in an individual – autism seems to be the most frequent referral we get with this indication.
- Finding whether there are any identical genes that cause a diagnosis is not an easy task and requires techniques not covered by public testing. Our approach is to do whole genome sequencing (WGS) in an individual with this AOH finding and then sort through the regions (there can be millions in some cases) to see if we can find a set of genes that explain what is going on.
- We require that all referring providers and the parents/care providers understand that there will be a private cost to come to an answer in all circumstances. Appointments are only booked where we have documentation that this is understood. We don’t want parents / care providers waiting a long time for an appointment to only find out about this later.
12. What is your workup for autism?
- Our focus is to look for genetic causes of autism (or related disorders like autism spectrum disorder) that has already been diagnosed.
- An increasing number of genetic syndromes are ultimately being found to be a cause of autism
- The typical practice is to start with a chromosomal microarray first (CMA). Sometimes fragile X testing is ordered if criteria are met. We ask that any of these tests, as decided by the referring doctor, be completed prior to referring to M.A.G.I.C.. If the results are positive or can’t be explained by the ordering physician then we will take the referral to explain abnormal results. In many cases, abnormal results from a CMA do not explain why a person has autism. A larger number of cases can be diagnosed using WGS. This means for the majority of people with autism, the approach through our clinic will be WGS. The purpose of running any test is to provide you with the best interpretation we can and not simply to run ‘a test’. We analyze the data from WGS before reporting it out. It’s important to understand that this is a different approach than most clinics and is aimed at being as comprehensive as possible. Without the right information, it’s not possible to draw the right conclusion. We do not order whole exome sequencing (WES) or gene panels as a general screen for genetic causes of autism. We also do not order testing, public or private, where we are not provided the raw sequencing data or from a lab that has not been traditionally involved in using this type of technology to make a genetic diagnosis.
- If you are a couple with a child with autism for which there is no genetic diagnosis and you are wondering whether there is a higher risk of having another child with autism, in general there is a higher risk but the percentage risk can vary depending on whether or not there is a genetic diagnosis. Prenatal testing is only possible in another pregnancy if a genetic cause has been identified. We require that the referring HCP discuss this with their patients and only accept referrals where there an interest in pursuing a genetic diagnosis.
- We are not a clinic that will diagnose autism. A specialist in autism, such as a neurodevelopmental pediatrician or psychologist, should be seen for that purpose. Our focus is trying to identify whether there is a genetic cause of autism with or without other neurodevelopmental issues.
- We do not order testing for folate receptor antibodies or prescribe folinic acid for these purposes. Our opinion is that the science behind this is not well developed enough yet to take this approach.
- If a referral is declined, it is generally because it was not understood whether the goal of the referral fits in with this scope or whether this was communicated to the patient or care providers.
13. What evaluation do you offer during pregnancy?
- Consultations during pregnancy are handled as a priority. We will accept self-referrals for pregnancy depending on the circumstances.
- The following are our primary services in pregnancy:
- Non-Invasive prenatal screening (NIPS) which is a private test. The cost is for the test only. The consultation is covered by the insurance provider with the conditions as described above under the FAQ for consultations.
- Medical Genetics consultation for fetal anomalies or genetic diseases affecting the pregnancy – whether the mother has or is considered to have a genetic disease or the baby. Examples of a mother’s genetic disease can include homocystinuria. Examples of fetal anomalies can include absence of a limb on fetal ultrasound. There is no fee for the consultation (same conditions as a general consultation) but there are certain tests that may not be publicly covered (such as WGS on an amniocentesis sample) which would be at a private cost if chosen. Other types of tests, like fetal karyotyping, are covered by public services and we will arrange and order them as indicated.
- Arranging for invasive prenatal testing using chorionic villus sampling or amniocentesis if the pregnancy is at risk for a metabolic or genetic disease.
- Pre-pregnancy screening for genetic diseases in the couple considering a pregnancy. The approach will be customized to the situation. For example, screening for thalassemia may be done through public testing if it meets the public testing conditions. We do offer WGS carrier screening for couples as a private test.
14. What about services like nursing, genetic counselling or pharmacy consultation?
- Registered nurses, genetic counsellors and pharmacists are professionals in their own right however there is no public coverage for these services – the services will be billed directly to the patient
- If one of these professionals is involved in the initial consultation, they will help set up requisitions for bloodwork or imaging as part of the initial consultation without a charge but any additional services, such as answering emails, telephone requests, medical advice will be billed directly to the patient
What are the typical types of patients seen at M.A.G.I.C. Clinic?
All of the testing we run in our laboratory, Discovery DNA, or send to other laboratories, such as Alberta Precision Laboratories or others, is clinic-grade testing in certified labs that have considerable experience, and the results can specifically be used to make a diagnosis. We place a high priority on quality, certification and accreditation and being as comprehensive as we can provide our interpretation on whether or not a genetic diagnosis exists rather than you have to keep doing more tests in the future in search of a genetic diagnosis. We do not rely on tests, whether ordered by other doctors or as direct-to-consumer tests, to make a diagnosis that do not meet these quality requirements.
1. Patients with a pre-existing metabolic or genetic disease
Patients with a pre-existing metabolic or genetic disease that fits within our scope of care. Examples of metabolic diseases include Fabry disease, Gaucher disease, Hurler syndrome, Hunter syndrome, Pompe disease (and other lysosomal storage diseases), urea cycle diseases, methyl-malonic acidemias, homocystinurias, mitochondrial diseases and the list goes on for about 400 diseases. Examples of genetic diseases include chromosomal conditions (like 22q11 microdeletion or Down syndrome but there are hundreds), single gene disorders (there are thousands). It’s basically many of the things you will find in OMIM. We do not see common findings on genetic testing like MTHFR common population variants or many of the popular direct-to-consumer type findings.
2. Children and adults with chronic conditions that have a high index of suspicion for a rare genetic disease
Children and adults with chronic conditions that have a high index of suspicion for a rare genetic disease for the purpose of trying to get a diagnosis. This can include things like developmental delay, early onset hearing loss, ataxia, muscle diseases, neurological diseases that have a genetic basis, autoimmune diseases, heart diseases, kidney diseases, bone diseases, eye diseases and many others.
3. Patients needing Whole Genome Sequencing (WGS)
Patients needing Whole Genome Sequencing (WGS) to diagnose a genetic disease. This is a private test (described in other FAQs). We provide consultation for and interpret the test results. WGS is ordered as medically indicated. We do not offer any test, public or private, if not medically indicated. We realize opinions can differ. WGS can be ordered if consultation is not required by you or your provider at https://www.discoverydna.ca . The quality of different WGS can differ among different companies. If you are looking to see if there is a diagnosis based on a WGS, we will interpret the reported finding as best we can from selected laboratories we have experience with such as Discovery DNA (our laboratory), Blueprint Genetics, Prevention Genetics, GeneDx, and Centogene. It is possible the test you previously had done was a research test – we do not provide interpretation of research tests. In many cases where there may have been publicly paid testing through one of these laboratories, the findings are based on older technologies, analyses or unclear findings and a new test may be required that does not qualify for public funding as a retest. The goal is to do genomic sequencing once and only once.
4. Pharmacogenomics testing and interpretation
Pharmacogenomics testing and interpretation. This is a private test. Our service is mainly through testing in our lab at discoverydna.ca. The test can be ordered by you or your care provider directly. If there is a medical issue that requires physician interpretation then we will consider a consultation from your health care provider. Because of the nature of these tests, and that the quality is not regulated, we do not provide medical consultation for pharmacogenomics testing done through outside labs.
5. Skin biopsies as a stand alone test
Skin biopsies as a stand alone test. This approach depend on the indication. This is a minor surgical procedure done with local freezing in clinic. It may be used to test for a variety of metabolic diseases, as a surrogate for a muscle biopsy if a muscle biopsy is too high of a risk (a skin biopsy cannot run all the tests nor it as good as a muscle biopsy for mitochondrial disease though and cannot test mtDNA), for neuronal ceroid lipofuscinosis and small fibre neuropathy (small fibre neuropathy is a private test sent out of province since it will not be analyzed for such in Alberta).
6. Mitochondrial disease diagnosis
Mitochondrial disease diagnosis. Diagnosing mitochondrial disease is complex. We have 2 basic groups of genes: one set of genes we inherit from both parents (inside the nucleus of the cell) and the second group are inside the mitochondrial of the cell and inherited only from the mother. The genes in the nucleus are nuclear DNA (nDNA) and the genes in the mitochondria are on mitochondrial DNA (mtDNA). Only a small set of genes are on mtDNA. Most mitochondrial diseases are still due to genes on nDNA – the most comprehensive way to screen for these diseases is whole genome sequencing (WGS). Our approach, based on our own published work and that of many others, uses a WGS-first approach, especially in children, to screen for mitochondrial diseases. This is a private test but it is non-invasive (needing a check swab, saliva or sometimes blood/urine). If the WGS is negative and there still is a high index of suspicion for a mitochondrial disease, we would next consider our Invasive Mitochondrial testing protocol which involves a muscle biopsy plus skin biopsy plus lumbar puncture. If the Invasive Mitochondrial testing protocol is to be used, the goal is to do it once and only once. Patient risk factors are also taken into account so the test must meet all conditions before it is performed. A muscle biopsy is still the gold standard to look for many mitochondrial diseases especially when WGS is negative. Muscle biopsy is an invasive test – this will require a piece of muscle tissue from the thigh. This tissue will not be regenerated in the patient and is a permanent loss of tissue. For adults muscle biopsy is done with local freezing in clinic. For children, we will need to do the muscle biopsy as a minor surgical procedure in a hospital with anesthesia (as permitted by hospital privileges). There is a risk of bleeding and/or infection from a muscle biopsy. Small children have a smaller amount of muscle so removing muscle can have implications for muscle function later in life. While we have performed hundreds of muscle biopsies safely, for each patient this is a serious consideration and we will only consider it if WGS is negative and a muscle biopsy is needed to identify a mitochondrial diseases. Provinces have different services they will pay for tests from a muscle biopsy and certain tests are not paid for if a patient is out of province. The medical procedure is covered (limitations above) but there is a charge for consumables (such as dry ice) and transport for which there is a fee. For patients that don’t require anesthesia, needle muscle biopsy is performed in clinic. Local freezing may help take the edge off the pain but there will still be some pain from the procedure which may linger for weeks or longer. If anesthesia is required, there may be restrictions in using hospital services for out of province patients that are beyond our control. In our experience, based on hundreds of procedures and outcomes, the following is the most comprehensive method to diagnose a mitochondrial disease. Our mitochondrial invasive testing protocol includes:
-
- Muscle Biopsy with Tissue Analysis using microscopy performed by APL – publicly covered for patients with Alberta health insurance.
- Muscle mtDNA analysis using Southern blot and long range PCR performed by APL – publicly covered for patients with Alberta health insurance
- Muscle Blue native polyacrylamide gel electrophoresis (BN-PAGE) and mitochondrial electron transport chain activity to a lab in the United States – publicly covered for patients with Alberta health insurance. For out of province patients, this muscle biopsy analysis is not covered. Please note that Southern blot and long range PCR do not typically give precise breakpoints for mitochondrial deletions.
- Muscle Nanopore long read mtDNA sequencing through our laboratory, Discovery DNA – this is a private test but available to all patients from every province. Nanopore sequencing can give a more precise breakpoints but does come at a private cost. Nanopore sequencing is performed on all muscle biopsies since, in our experience, sometimes Southern blot or long range PCR will not provide a diagnosis because of the larger tissue requirement and due to the invasive nature of the procedure, we perform Nanopore sequencing on all samples to avoid having to re-do the muscle biopsy.
- Lumbar Puncture. As a routine procedure along with a muscle biopsy, we also perform a lumbar puncture. This takes some fluid from the lower part of the spine to analyze for abnormal cerebrospinal fluid (CSF) levels of 5-MTHF and neurotransmitters. Low levels of 5–MTHF have been found in some patients with mitochondrial disease and in that case we would advise treatment with folinic acid. While getting coverage for folinic acid treatment is challenging in the best of circumstances, in our experience it helps if we can demonstrate how CSF levels of 5-MTHF. Lumbar puncture does have a risk of post-spinal headache, bleeding, infection and sometimes the need for a blood patch. We do not provide shortcuts around the testing once invasive procedures are done by using other types of testing even if they are publicly covered (such as short read mtDNA sequencing). A skin biopsy is also done as a routine procedure since this may be needed for confirmation of muscle test results, we may not get enough muscle to run all the needed tests and because some tests may need skin as the primary test. The skin is usually stored until needed.
- Skin is removed from the site of the muscle biopsy (about the size of a fingernail clipping) with no major increase in overall risk.
7. Cytokine testing: 95 Plex and similar
Cytokine testing: 95 Plex and similar. Cytokines are peptides in the blood that can have abnormal ranges in certain inflammatory conditions and responses. We use a local lab for cytokine testing. This is a private test. We are not a primary immunology or rheumatology clinic. To order this testing, there has to be a request from a specialist or, as part of the consultation, it may be that this test can help distinguish between an immunologic, inflammatory versus a genetic cause for a patient’s issues. These are tests that require quite a bit of interpretation which is not an exact science at this stage and in certain rare circumstances they may be helpful. They are offered when these circumstances apply.
8. Clinical trials
Clinical trials. You can be referred if you would like to participate in a clinical trial. You may not need to be a clinic patient in order to be part of a clinical trial especially if you have your own specialist. Participation in clinical trials is open to all patients regardless of their province of origin. If your health insurance is not valid in Alberta, you will need to get separate health insurance on your own. Clinical trial companies typically provide coverage for expenses like travel and accommodation when these are needed as part of a clinical trial. Coverage varies from one trial to the next. These will be outlined by the research coordinator assigned for each specific clinical trial.
1. Patients with a pre-existing metabolic or genetic disease
Patients with a pre-existing metabolic or genetic disease that fits within our scope of care. Examples of metabolic diseases include Fabry disease, Gaucher disease, Hurler syndrome, Hunter syndrome, Pompe disease (and other lysosomal storage diseases), urea cycle diseases, methyl-malonic acidemias, homocystinurias, mitochondrial diseases and the list goes on for about 400 diseases. Examples of genetic diseases include chromosomal conditions (like 22q11 microdeletion or Down syndrome but there are hundreds), single gene disorders (there are thousands). It’s basically many of the things you will find in OMIM. We do not see common findings on genetic testing like MTHFR common population variants or many of the popular direct-to-consumer type findings.
2. Children and adults with chronic conditions that have a high index of suspicion for a rare genetic disease
Children and adults with chronic conditions that have a high index of suspicion for a rare genetic disease for the purpose of trying to get a diagnosis. This can include things like developmental delay, early onset hearing loss, ataxia, muscle diseases, neurological diseases that have a genetic basis, autoimmune diseases, heart diseases, kidney diseases, bone diseases, eye diseases and many others.
3. Patients needing Whole Genome Sequencing (WGS)
Patients needing Whole Genome Sequencing (WGS) to diagnose a genetic disease. This is a private test (described in other FAQs). We provide consultation for and interpret the test results. WGS is ordered as medically indicated. We do not offer any test, public or private, if not medically indicated. We realize opinions can differ. WGS can be ordered if consultation is not required by you or your provider at https://www.discoverydna.ca . The quality of different WGS can differ among different companies. If you are looking to see if there is a diagnosis based on a WGS, we will interpret the reported finding as best we can from selected laboratories we have experience with such as Discovery DNA (our laboratory), Blueprint Genetics, Prevention Genetics, GeneDx, and Centogene. It is possible the test you previously had done was a research test – we do not provide interpretation of research tests. In many cases where there may have been publicly paid testing through one of these laboratories, the findings are based on older technologies, analyses or unclear findings and a new test may be required that does not qualify for public funding as a retest. The goal is to do genomic sequencing once and only once.
4. Pharmacogenomics testing and interpretation
Pharmacogenomics testing and interpretation. This is a private test. Our service is mainly through testing in our lab at discoverydna.ca. The test can be ordered by you or your care provider directly. If there is a medical issue that requires physician interpretation then we will consider a consultation from your health care provider. Because of the nature of these tests, and that the quality is not regulated, we do not provide medical consultation for pharmacogenomics testing done through outside labs.
5. Mitochondrial disease diagnosis
Mitochondrial disease diagnosis. Diagnosing mitochondrial disease is complex. We have 2 basic groups of genes: one set of genes we inherit from both parents (inside the nucleus of the cell) and the second group are inside the mitochondrial of the cell and inherited only from the mother. The genes in the nucleus are nuclear DNA (nDNA) and the genes in the mitochondria are on mitochondrial DNA (mtDNA). Only a small set of genes are on mtDNA. Most mitochondrial diseases are still due to genes on nDNA – the most comprehensive way to screen for these diseases is whole genome sequencing (WGS). Our approach, based on our own published work and that of many others, uses a WGS-first approach, especially in children, to screen for mitochondrial diseases. This is a private test but it is non-invasive (needing a check swab, saliva or sometimes blood/urine). If the WGS is negative and there still is a high index of suspicion for a mitochondrial disease, we would next consider our Invasive Mitochondrial testing protocol which involves a muscle biopsy plus skin biopsy plus lumbar puncture. If the Invasive Mitochondrial testing protocol is to be used, the goal is to do it once and only once. Patient risk factors are also taken into account so the test must meet all conditions before it is performed. A muscle biopsy is still the gold standard to look for many mitochondrial diseases especially when WGS is negative. Muscle biopsy is an invasive test – this will require a piece of muscle tissue from the thigh. This tissue will not be regenerated in the patient and is a permanent loss of tissue. For adults muscle biopsy is done with local freezing in clinic. For children, we will need to do the muscle biopsy as a minor surgical procedure in a hospital with anesthesia (as permitted by hospital privileges). There is a risk of bleeding and/or infection from a muscle biopsy. Small children have a smaller amount of muscle so removing muscle can have implications for muscle function later in life. While we have performed hundreds of muscle biopsies safely, for each patient this is a serious consideration and we will only consider it if WGS is negative and a muscle biopsy is needed to identify a mitochondrial diseases. Provinces have different services they will pay for tests from a muscle biopsy and certain tests are not paid for if a patient is out of province. The medical procedure is covered (limitations above) but there is a charge for consumables (such as dry ice) and transport for which there is a fee. For patients that don’t require anesthesia, needle muscle biopsy is performed in clinic. Local freezing may help take the edge off the pain but there will still be some pain from the procedure which may linger for weeks or longer. If anesthesia is required, there may be restrictions in using hospital services for out of province patients that are beyond our control. In our experience, based on hundreds of procedures and outcomes, the following is the most comprehensive method to diagnose a mitochondrial disease. Our mitochondrial invasive testing protocol includes:
-
- Muscle Biopsy with Tissue Analysis using microscopy performed by APL – publicly covered for patients with Alberta health insurance.
- Muscle mtDNA analysis using Southern blot and long range PCR performed by APL – publicly covered for patients with Alberta health insurance
- Muscle Blue native polyacrylamide gel electrophoresis (BN-PAGE) and mitochondrial electron transport chain activity to a lab in the United States – publicly covered for patients with Alberta health insurance. For out of province patients, this muscle biopsy analysis is not covered. Please note that Southern blot and long range PCR do not typically give precise breakpoints for mitochondrial deletions.
- Muscle Nanopore long read mtDNA sequencing through our laboratory, Discovery DNA – this is a private test but available to all patients from every province. Nanopore sequencing can give a more precise breakpoints but does come at a private cost. Nanopore sequencing is performed on all muscle biopsies since, in our experience, sometimes Southern blot or long range PCR will not provide a diagnosis because of the larger tissue requirement and due to the invasive nature of the procedure, we perform Nanopore sequencing on all samples to avoid having to re-do the muscle biopsy.
- Lumbar Puncture. As a routine procedure along with a muscle biopsy, we also perform a lumbar puncture. This takes some fluid from the lower part of the spine to analyze for abnormal cerebrospinal fluid (CSF) levels of 5-MTHF and neurotransmitters. Low levels of 5–MTHF have been found in some patients with mitochondrial disease and in that case we would advise treatment with folinic acid. While getting coverage for folinic acid treatment is challenging in the best of circumstances, in our experience it helps if we can demonstrate how CSF levels of 5-MTHF. Lumbar puncture does have a risk of post-spinal headache, bleeding, infection and sometimes the need for a blood patch. We do not provide shortcuts around the testing once invasive procedures are done by using other types of testing even if they are publicly covered (such as short read mtDNA sequencing). A skin biopsy is also done as a routine procedure since this may be needed for confirmation of muscle test results, we may not get enough muscle to run all the needed tests and because some tests may need skin as the primary test. The skin is usually stored until needed.
- Skin is removed from the site of the muscle biopsy (about the size of a fingernail clipping) with no major increase in overall risk.
6. Skin biopsies as a stand alone test
Skin biopsies as a stand alone test. This approach depend on the indication. This is a minor surgical procedure done with local freezing in clinic. It may be used to test for a variety of metabolic diseases, as a surrogate for a muscle biopsy if a muscle biopsy is too high of a risk (a skin biopsy cannot run all the tests nor it as good as a muscle biopsy for mitochondrial disease though and cannot test mtDNA), for neuronal ceroid lipofuscinosis and small fibre neuropathy (small fibre neuropathy is a private test sent out of province since it will not be analyzed for such in Alberta).
7. Cytokine testing: 95 Plex and similar
Cytokine testing: 95 Plex and similar. Cytokines are peptides in the blood that can have abnormal ranges in certain inflammatory conditions and responses. We use a local lab for cytokine testing. This is a private test. We are not a primary immunology or rheumatology clinic. To order this testing, there has to be a request from a specialist or, as part of the consultation, it may be that this test can help distinguish between an immunologic, inflammatory versus a genetic cause for a patient’s issues. These are tests that require quite a bit of interpretation which is not an exact science at this stage and in certain rare circumstances they may be helpful. They are offered when these circumstances apply.
8. Clinical trials
Clinical trials. You can be referred if you would like to participate in a clinical trial. You may not need to be a clinic patient in order to be part of a clinical trial especially if you have your own specialist. Participation in clinical trials is open to all patients regardless of their province of origin. If your health insurance is not valid in Alberta, you will need to get separate health insurance on your own. Clinical trial companies typically provide coverage for expenses like travel and accommodation when these are needed as part of a clinical trial. Coverage varies from one trial to the next. These will be outlined by the research coordinator assigned for each specific clinical trial.
About Us
M.A.G.I.C. stands for Metabolics and Genetics in Canada. We are a medical clinic that specializes in looking after patients (children and adults) with rare diseases that are due to changes in their DNA.
Want to Learn More?
Reach a Team that cares about you
Get In Touch: